Why it is important
Intrahepatic cholestasis of pregnancy (ICP) is the most common liver disorder specific to pregnancy. In the UK, it affects approximately 1 in 160 pregnant women and is particularly common in those of South Asian ethnicity. The prevalence of ICP varies globally; it is especially common in the Andean nations of Latin America, affecting up to 3% of pregnant women in Chile. ICP typically presents with symptoms of itching in pregnant women and is associated with abnormal liver blood tests. The most specific blood test to diagnose ICP is serum bile acid measurement, which is crucial because women with high serum bile acid concentrations are at increased risk of adverse pregnancy outcomes, including spontaneous preterm birth and stillbirth. 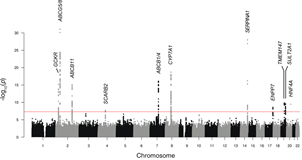 Affected women are also at increased risk of liver/gallbladder disease in later life. Their children face an elevated risk of increased adiposity, high cholesterol/dyslipidaemia, and insulin resistance.
Affected women are also at increased risk of liver/gallbladder disease in later life. Their children face an elevated risk of increased adiposity, high cholesterol/dyslipidaemia, and insulin resistance.
Summary of current research
Causes of ICP: We study the genetic factors that cause women to be susceptible to ICP. Approximately 25% of women have pathogenic mutations in genes that influence bile acid transport in the liver (principally ABCB4/MDR3 and ABCB11/BSEP). We have also shown that common genetic variants increase the likelihood of developing ICP. Current research is focusing on the interaction between different susceptibility variants and whether the same genetic changes are responsible for the onset of ICP in people of different ethnic backgrounds.
We and others have shown that the high concentrations of oestrogen and progesterone metabolites found in pregnancy can affect the liver’s metabolism and transport of bile acids, leading to cholestasis in susceptible individuals. Current research uses in vivo an in vitro models to study how reproductive hormones influence susceptibility to cholestasis. We are also investigating whether specific therapies can protect against the impact of reproductive hormones on cholestasis (or the production of metabolites that cause itching). Women with ICP have metabolic disturbances (e.g. dyslipidaemia/hyperglycaemia). We are studying potential mechanisms to explain the metabolic abnormalities found in women with ICP.
To understand the causes of preterm birth and stillbirth in ICP, we use in vivo and in vitro models. Key current results and future focus include examining how drugs that block bile acid uptake from the gut can protect against cholestasis, itching, preterm birth, and fetal loss. Using cell models of the myometrium, we study how bile acids induce contractions and whether specific drugs, such as ursodeoxycholic acid (UDCA), can prevent these changes, potentially protecting against preterm birth.
We also study pregnant women with ICP, comparing findings to pregnant controls without ICP. Key results include demonstrating a relationship between maternal serum bile acid concentrations and abnormalities in fetal heart rhythm, as well as showing that UDCA can prevent some of these changes. We have used wearable monitors of the fetal electrocardiogram (fECG) to evaluate heart rhythm changes, and future work will examine fECG changes in other conditions that may be complicated by stillbirth, including diabetes mellitus and long QT syndrome.
How the research benefits patients
We have collaborated with the charity ICP Support since its inception to ensure that our work is relevant to patient needs. When new research ideas emerge (including those proposed by women linked to the charity), we arrange focus groups, surveys, and peer reviews of research proposals with the charity’s help.
Specific examples of the ways our research has benefited patients include:
- Demonstration that serum bile acid measurement is the most reliable test to predict pregnancies at risk of stillbirth and spontaneous preterm birth.
- Evidence that serum bile acids should be checked using non-fasting blood samples to avoid missing the peaks associated with an increased risk of adverse pregnancy outcomes.
- Meta-analysis showing that ursodeoxycholic acid protects against spontaneous preterm birth in singleton pregnancies.
- The development of a cholestasis gene panel to identify pathogenic mutations in approximately 25% of women with severe, early-onset ICP.
Researchers
- Jenny Chambers
- Pete Dixon
- Alice Mitchell
- Caroline Ovadia
- Josca Mariette Schoonejans
- Anna Yang
- Julia Zollner