New treatments could stop multiple sclerosis progression for the first time
by Sam Wong

Thanks to research on brains donated by MS patients, Imperial researchers have made major advances in efforts to understand and treat the disease.
Around 100,000 people in the UK have multiple sclerosis and, while several treatments exist to treat early attacks, there is currently nothing to stop the disease from progressing. Over the last decade, Imperial scientists have contributed to major advances in our understanding of the condition by studying post-mortem brain tissue. Now they are taking new treatment strategies to patients for the first time.
Walking along a beach while on holiday in Devon with her sister in 1996, Jane began to feel pins and needles in her feet. As she trod on the stones, the tingling became painful, and it became clear that something was wrong. When she returned home, the pain went away, but three weeks later it came back. Her doctor sent her for tests at Charing Cross Hospital. A few months later, at the age of 38, she was told she had multiple sclerosis (MS).
“It was the end of the world when I was first diagnosed,” she says. She didn’t tell her children at first because she didn’t want them to be worried. “When I got the blue badge for the car, they said, ‘why do you have this? There’s nothing wrong with you.’” Gradually, her legs grew more unsteady and walking became more difficult.
Sixteen years on, Jane can still walk but she relies on the aid of a stick. Working from her home in west London, she keeps up a successful career as a journalist, but travelling to meet people becomes harder each year. Her appearance is healthy and her demeanour positive, but the disease, and the knowledge that it will continue to get worse, can’t escape her mind for long.
“I do think about it every day and have done since I was diagnosed,” she says. “It stops you thinking about the future in a warm comfortable way, or being able to picture the ‘Saga poster old age’, which is a loss. It’s a sort of bereavement.”
Friendly fire
Jane’s symptoms are the result of her brain coming under attack from her own immune system. Her immune cells, whose job is to protect her body against microbial invaders, have instead set their sights on a fatty substance called myelin, which wraps around her nerve fibres. Gradually they are tearing apart this myelin insulation, leaving her neurons unable to carry electrical signals efficiently. The reason for the attacks is still a mystery.
Most sufferers start to experience symptoms between the ages of 18 and 40. Many drugs designed to quell the immune system are available to prevent attacks in the early phase of the disease, known as relapsing-remitting MS, but Jane has entered the phase called secondary progressive MS, in which symptoms steadily get worse. So far no treatment has yet been shown to prevent the slow progression of disease that might eventually mean she has to use a wheelchair.
That could be about to change. Jane has just had her first infusion in a clinical trial being run by Imperial researchers in the MS clinic at Charing Cross Hospital, part of Imperial College Healthcare NHS Trust. She was either given the drug Tysabri (natalizumab) or the control, a saline solution, but neither she nor her doctor knows which.
“People told me you can tell if you’re getting the drug because it just feels different,” she says. “Obviously I hope I’m not on a placebo, but I didn’t really feel anything or notice any side effects.
Keeping immune cells at bay
Tysabri is already approved for treating early attacks of MS, but it’s still unclear how these attacks are related to progression of the disease or whether this drug could help at later stages. The trial has been based on results of research by Professor Richard Reynolds’ group, at Imperial’s Hammersmith Campus, which offer clues as to why MS progresses.
“The early attacks of MS seem to involve a rapid influx of immune cells into different parts of the brain,” Richard says. These cells normally circulate in the bloodstream, moving out when they are summoned to sites of infection. In MS, they migrate in large numbers into the brain and cause inflammation. The cells must first stick to the blood vessel wall before they can pass through it into the brain. In these early stages, Tysabri works by stopping immune cells from sticking to the walls of blood vessels.
By looking at post-mortem brain tissue donated by patients, Richard’s team discovered that in the later stages of MS, the inflammation is no longer caused by immune cells moving from the bloodstream into the brain, but by immune cells that are trapped in the tissues that surround the brain and in the brain itself. “The data suggest that if we can dampen those cells down and stop their movement once they get into the brain, we might stop that slow progression,” he says. “We need to see whether Tysabri can also do this, and in two years’ time we should know whether or not it works.”
Knowledge bank
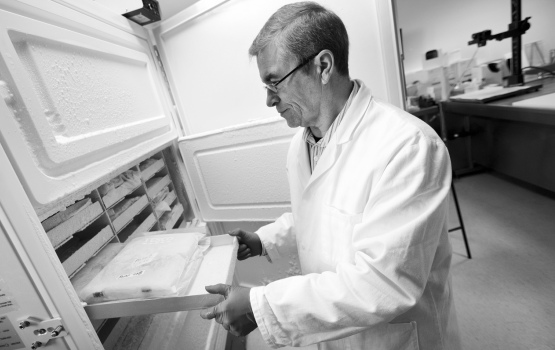
To find out what goes wrong in the brain of an MS patient, you need to look inside it. Richard has been collecting brains since 1998, when the MS Society funded him to set up a tissue bank at Imperial. He and his colleagues travelled the country, meeting groups of patients and their families, asking them to consider donating their organs for science when they die.
“I think we’ve visited something like 170 groups over the years,” he says. “We go and tell them about the research that’s going on in MS, how it’s helping develop new drug treatments and why we need human tissue to do that.”
The response has been extremely supportive. “We found that people with MS and their families are very much behind this idea. They don’t think, ‘ooh no, I can’t do that’. They’re hungry for knowledge and they want to contribute to that knowledge.”
A similar scheme was set up by Parkinson’s UK a few years later, and now the collection for the two diseases together numbers more than 1,000 brains, making it one of the largest in the world. Almost 10,000 more people have pledged to give their brains, ensuring a steady supply of about three brains a week. The brain tissue isn’t just used for research at Imperial; it’s also sent around the world to enable other scientists working on MS and Parkinson’s to study.
Loss of nerve
The insights gained from studying these specimens have been significant. It’s now clear that far from being simply a disease of the nerve fibres’ myelin coating, there is also extensive damage to the nerve cells themselves.
“When we cut sections of the brain and actually count the neurons in various parts of the brain tissue, we can see that the numbers have reduced quite substantially,” Richard says. This loss of nerve cells is called neurodegeneration, which is a feature that is common to Alzheimer’s, Parkinson’s, and motor neurone disease.
“It’s very much changing the way we think about how the disease progresses over time and how we can treat it. Most of the drug treatments that are available now, based on the previous 10 years’ research, are drugs that dampen down the inflammation in the brain – what are called immune-modulatory drugs. Instead, we’re now beginning to think about how to protect the neurons from degeneration, which is something that’s really just started for MS.”










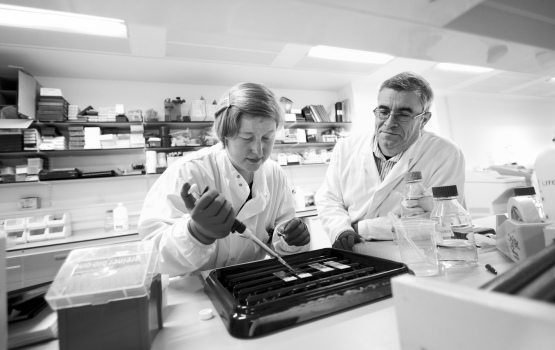









This neurodegeneration is clear when you look at a brain under the microscope, but doctors don’t have the luxury of being able to take out slices of brain from living patients. Richard and others at Imperial are therefore working on non-invasive ways to measure the number of neurons in different areas of the brain, using advanced imaging techniques. Recently they have begun to experiment with scanning donated brains, as they would a patient’s brain, before cutting them into slices. Researchers can then compare the scans with what they see in the slices to help them interpret the imaging data.
Another line of investigation is looking at molecular changes in the MS brain. Modern genetic techniques allow researchers to look at how all 30,000 human genes were either turned on or off at the moment when the patient died. They can also compare the levels of specific molecules in brains from people who died younger with levels in the brains of people who had milder disease and lived much longer. “We can now say that, in people whose disease progressed more rapidly, certain molecules are increased in the brain in areas of damage,” Richard says. “This has now enabled us to set up experimental systems where we can change the levels of the protein up or down to see if that molecule is involved in causing the damage, which helps towards developing new therapies.”
Rebooting the immune system
Richard estimates that there are about 100 drugs for MS in clinical trials right now, compared with fewer than 10 a decade ago. In addition to these drug trials, some researchers are investigating a more radical approach: obliterating the immune system with chemotherapy or radiation, and replacing the misfiring cells with new ones grown from a patient’s own stem cells. One of those researchers is neuroimmunologist Dr Paolo Muraro, also based on the Hammersmith Campus.
“We call this ‘rebooting’ the immune system because it essentially aims to start the immune system anew,” he says. “The hope is that any aberrant immune cells that have developed in the MS patient would be wiped out by the immunosuppression and would not be regenerated and, therefore, there would be a prolonged remission from any inflammation. Hopefully lifelong, but we don’t know yet.”
So far, around 600 patients worldwide have had this treatment in small trials. The results for patients with early-stage MS have been promising, but the safety and efficacy of the procedure is still being established. Paolo is now working with an international team of scientists to devise a protocol for a major trial that would give a more definitive answer.
The type of stem cells that replace the harmful immune cells are called haematopoietic stem cells (HSCs). They’re found in the bone marrow, but they also circulate in the blood in low numbers. Some drugs, including Tysabri, seem to increase the numbers of HSCs in the blood in some patients, and it’s been suggested that mobilising stem cells in this way could help tissues to repair themselves.
A recent study by Paolo’s group found that patients whose circulating HSCs increase in response to Tysabri have fewer relapses, less disability, and fewer brain lesions visible on MRI scans compared with those who don’t respond to the drug in this way. The reason for this is unclear, but if this observation is confirmed in larger studies, it could be a useful personal indicator of the drug’s success. For instance, doctors might consider taking a patient off treatment if the numbers of stem cells in their blood don’t increase.
Nurturing chemicals
HSCs are one of two types of stem cells that reside in the bone marrow. The other, mesenchymal stem cells (MSCs), are another promising treatment possibility. They form a supportive tissue that shelters the HSCs in the bone marrow, but they can also be taken out and grown in culture to large numbers. Scientists initially thought that they could transform into new neurons or new myelin-producing cells and replace cells that were damaged in the MS brain. It turned out that this didn’t happen, but they did demonstrate a number of other properties that could make them useful in treatment.
They actually produce a range of chemical factors, some of which alter the behaviour of immune cells, and some of which protect nerve cells and encourage repair. “The idea,” explains Paolo, “is that by taking MSCs from the bone marrow, growing them to large numbers and giving them back to a patient, we could aim to reduce the inflammation, or hopefully stop it. Even without turning themselves into other cells, they could still help in another way.”
Paolo’s group is about to start giving MSC treatment to patients in the UK arm of a trial that will involve a total of 150 patients across Europe. It will be five years before the results are known.
Intelligent therapy
Some scientists think that stem cell therapies, while informative about possible mechanisms for repair in the brain, are too complex and expensive to ever be used widely. But Paolo believes the costs will come down as technology improves, and that cells have certain qualities that make them a more intelligent therapy than drugs could ever be.
“It’s possible and desirable that we could gain a detailed knowledge of what cells do, isolate molecules that they produce and deliver them in drugs,” he says. “But one thing that would be hard to replicate with conventional drug therapy is the fact that certain cells used in cell therapies, such as MSCs, have a so-called therapeutic plasticity. This means that the cells adapt their behaviour depending on the environment that they are in.”
Some studies have shown evidence that the more inflammation there is in the body, the more MSCs suppress the immune system. “They don’t just switch on and off; they have a continuous variation in their biological behaviour. This makes them an order of magnitude more advanced in their refinement compared to any drug that we use. I don’t know if science will be able to replicate that.”
Into the unknown
Paolo and Richard work closely with the staff at the MS clinic at Charing Cross Hospital to get promising treatments from the lab to patients as quickly as possible. In the last four years, around 1,200 patients with MS have enrolled in research studies at Charing Cross. The director of the MS Clinical Trials Unit, Dr Richard Nicholas, sees finding new treatments as an integral part of his job as a clinician. “There are increasingly effective treatments for relapsing-remitting MS, but we can do little to help patients with secondary progressive MS,” he says. “You have to sit in front of people every day who are getting worse, so you constantly ask: ‘why can’t we do something about it?’”
This determination to improve patients’ lives leads him to a wide range of collaborators, at Imperial and beyond, whose ideas are ripe for clinical investigation. “We are one cog,” he says. “We work with people who are much cleverer than us.”
While some of the studies are showing promising results, inevitably, some don’t go so well. Such occasions are hugely disappointing for patients, scientists and funders, but no one is about to give up on looking for better treatments. Jane took part in a trial six years ago that was abandoned when the treatment proved ineffective. This time around, she has her fingers crossed that Tysabri might stop her getting worse, or perhaps even improve her condition.
Meanwhile, Richard Nicholas is working hard to recruit more volunteers who might benefit from Tysabri and contribute to our understanding of how it could be developed as an effective treatment. As ever in science, it’s a step into the unknown. “We’re learning – we’re at the front end of things. We take the patients with us”.
This article first appeared in Imperial Magazine, Issue 38. You can view and download a whole copy of the magazine, from www.imperial.ac.uk/imperialmagazine.
Article text (excluding photos or graphics) © Imperial College London.
Photos and graphics subject to third party copyright used with permission or © Imperial College London.
Reporter
Sam Wong
School of Professional Development