A novel study on Tumour Identification During Fluorescence Guided Breast Surgery
A Hamlyn-led project investigated the diagnostic accuracy in detecting tumours during breast conserving surgery by using intravenous indocyanine green
Breast conserving surgery (BCS) is currently the cornerstone treatment for early stage breast cancer as, when combined with radiotherapy, it offers equivalent cancer control to mastectomy but with improved quality of life outcomes.
However, BCS is associated with a greater risk of positive resection margins and re-operative intervention. On average, 21.% of women in the USA and 27% of women in the UK treated with BCS undergo a second operation because of close positive margins.
 Positive margins are a major challenge during BCS, as re-operation has negative sequelae to both the patient and healthcare system, resulting in poorer cosmetic outcome, increased psychological burden, delays to neoadjuvant treatment, and increasing treatment costs by approximately $2,360 per patient in the US and £2,136 per patient the UK.
Positive margins are a major challenge during BCS, as re-operation has negative sequelae to both the patient and healthcare system, resulting in poorer cosmetic outcome, increased psychological burden, delays to neoadjuvant treatment, and increasing treatment costs by approximately $2,360 per patient in the US and £2,136 per patient the UK.
In an attempt to decrease re-excision rates, a spectrum of technologies for intraoperative guidance has emerged. One of technologies is Fluorescence guided surgery (FGS).
FGS is an optical approach that capitalises on inherent or externally administered fluorescent molecules to identify targeted tissues. Tumour identification with fluorescence imaging could improve positive resection margin rates through demarcating location, size, and invasiveness of tumours.
A Novel Study on Tumour Identification During Fluorescence Guided Breast Surgery
In the light of this, a Hamlyn-led research team at the Hamlyn Centre investigated the FGS technique’s diagnostic accuracy in detecting tumours during BCS using intravenous indocyanine green (ICG) and a custom-built fluorescence camera system.

In this single-centre prospective clinical study, 40 recruited BCS patients were sub-categorised into two cohorts.
In the first ‘enhanced permeability and retention’ (EPR) cohort, 0.25 mg/kg ICG was injected * 25 min prior to tumour excision, and in the second ‘angiography’ cohort, * 5 min prior to tumour excision.
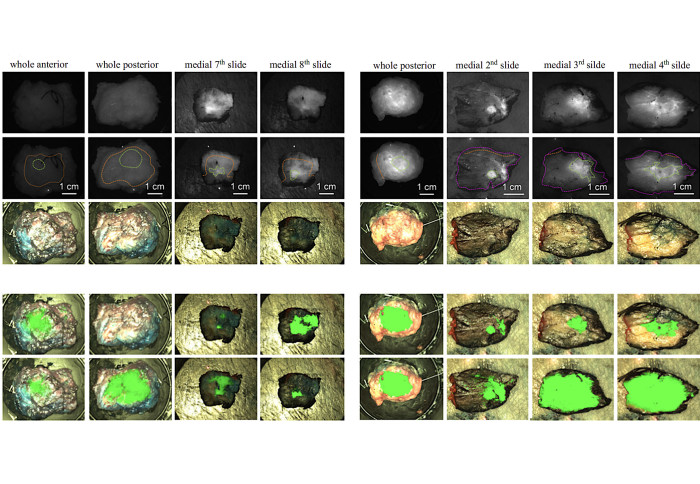
Subsequently, an in-house imaging system was used to image the tumour in situ prior to resection, ex vivo following resection, the resection bed, and during grossing in the histopathology laboratory to compare the technique’s diagnostic accuracy between the cohorts.
The research results showed that the two cohorts were matched in patient and tumour characteristics. The majority of patients had invasive ductal carcinoma with concomitant ductal carcinoma in situ.

Moreover, Tumour-to-background ratio (TBR) in the angiography cohort was superior to the EPR cohort (TBR = 3.18 ± 1.74 vs 2.10 ± 0.92 respectively, p = 0.023). Tumour detection reached sensitivity and specificity scores of 0.82 and 0.93 for the angiography cohort and 0.66 and 0.90 for the EPR cohort, respectively (p = 0.1051 and p = 0.9099).
In conclusion, ICG could be useful for macroscopic tumour evaluation during BCS, particularly when administered using short (*5 min), rather than longer (*25 min) intervals for injection prior resection. In other words, ICG administration timing during the angiography phase (compared with the EPR phase) could improve TBR and diagnostic accuracy.
In the near future, our research team plans to focus on image pattern analysis and adaptation of the camera system to targeting fluorophores specific to breast cancer.
Martha Kedrzycki, Maria Leiloglou, Vadzim Chalau, Nicolas Chiarini, Paul T. R. Thiruchelvam, Dimitri J. Hadjiminas, Katy R. Hogben, Faiza Rashid, Rathi Ramakrishnan, Ara W. Darzi, Daniel S. Elson, and Daniel R. Leff, "The Impact of Temporal Variation in Indocyanine Green Administration on Tumour Identification During Fluorescence Guided Breast Surgery", Annals of Surgical Oncology, 28, 5617–5625, August 2021.
Article supporters
Article text (excluding photos or graphics) © Imperial College London.
Photos and graphics subject to third party copyright used with permission or © Imperial College London.
Reporter
Erh-Ya (Asa) Tsui
Enterprise
Martha Kedrzycki
Department of Surgery & Cancer
Dr Maria Leiloglou
Department of Surgery & Cancer